CASE AUTH/2672/11/13 ANONYMOUS CONTACTABLE MEMBER OF THE PUBLIC v MERCK SHARP & DOHME
NO BREACH OF THE CODE
Clinical trial disclosure (Brinavess, Victrelis and Sycrest)
An anonymous contactable member of the public complained about the information published as ‘Clinical Trial Transparency: an assessment of the disclosure results of company-sponsored trials associated with new medicines approved recently in Europe’. The study was published in Current Medical Research & Opinion (CMRO) on 11 November 2013. The study authors were Dr B Rawal, Research, Medical and Innovation Director at the ABPI and B R Deane, a freelance consultant in pharmaceutical marketing and communications. Publication support for the study was funded by the ABPI.
The study surveyed various publicly available information sources for clinical trial registration and disclosure of results searched from 27 December 2012 to 31 January 2013. It covered 53 new medicines (except vaccines and fixed dose combinations) approved for marketing by 34 companies by the European Medicines Agency (EMA) in 2009, 2010 and 2011. It included all completed company-sponsored clinical trials conducted in patients and recorded on a clinical trial registry and/or included in a European Public Assessment Report (EPAR). The CMRO publication did not include the specific data for each product. This was available via a website link and was referred to by the complainant. The study did not aim to assess the content of disclosure against any specific requirements.
The complainant stated that the study detailed a number of companies which had not disclosed their clinical trial results in line with the ABPI for licensed products. The complainant provided a link to relevant information which included the published study plus detailed information for each product that was assessed.
The summary output for each medicine set out the sources for all trials found, irrespective of sponsor and an analysis of publication disclosure in the form of a table which gave details for the studies for Brinavess (vernakalant hydrochloride), Sycrest (asenapine) and Victrelis (boceprevir).
The detailed response from Merck Sharp & Dohme is given below.
General detailed comments from the Panel are given below.
With regard to Sycrest, the Panel noted that eight of the evaluable studies had not been disclosed in the timeframe. The disclosure percentage was 64%. The disclosure percentage at 31 January 2013 of trials completed before the end of January 2012 was 100%.
The Panel noted Merck Sharp & Dohme’s submission that Sycrest was first approved and commercially available around 13 August 2009. For studies completed before that date the 2008 Code applied and hence the Joint Position 2005 was relevant.
The Panel noted that one study completed in 2005. It was not clear when the results were posted or whether there was UK involvement. The study was a preference study of flavouring. The Panel considered that this study could be considered an exploratory trial and thus the results did not need to be disclosed under the Joint Position 2005 unless they were deemed to have significant medical importance and might have an impact on product labelling. The Panel was unsure whether the results were of significant medical importance. The complainant had not provided any details in this regard. The Panel considered that publication of such data was preferable however on the information before it there appeared to be no need to disclose the trial results under the 2008 Code. The Panel ruled no breach of the 2008 Code including Clause 2.
The Panel noted Merck Sharp & Dohme’s submission that the results of a study completed in December 2007 were presented at a meeting in June 2008 and posted in December 2009 immediately after the merger with Schering-Plough. The trial had UK sites. The Panel noted that the trial was on an indication unlicensed in the UK but schizophrenia was licensed in the US so the trial was covered by Joint Position 2005. The trial needed to be disclosed within one year of first approval and commercial availability of Sycrest ie before August 2010. On the information submitted by Merck Sharp & Dohme it appeared that this had been done as the study was posted in December 2009. The Panel therefore ruled no breach of the 2008 Code including Clause 2.
An anonymous contactable member of the public complained about the information published as ‘Clinical Trial Transparency: an assessment of the disclosure results of company-sponsored trials associated with new medicines approved recently in Europe’. The study was published in Current Medical Research & Opinion (CMRO) on 11 November 2013. The study authors were Dr B Rawal, Research, Medical and Innovation Director at the ABPI and B R Deane, a freelance consultant in pharmaceutical marketing and communications. Publication support for the study was funded by the ABPI.
The study surveyed various publicly available information sources for clinical trial registration and disclosure of results searched from 27 December 2012 to 31 January 2013. It covered 53 new medicines (except vaccines and fixed dose combinations) approved for marketing by 34 companies by the European Medicines Agency (EMA) in 2009, 2010 and 2011. It included all completed company-sponsored clinical trials conducted in patients and recorded on a clinical trial registry and/or included in a European Public Assessment Report (EPAR). The CMRO publication did not include the specific data for each product. This was available via a website link and was referred to by the complainant. The study did not aim to assess the content of disclosure against any specific requirements.
COMPLAINT
The complainant stated that the study detailed a number of companies which had not disclosed their clinical trial results in line with the ABPI for licensed products. The complainant provided a link to relevant information which included the published study plus detailed information for each product that was assessed.
The summary output for each medicine set out the sources for all trials found, irrespective of sponsor and an analysis of publication disclosure in the form of a table which gave details for the studies for each product.
The data for Brinavess (vernakalant hydrochloride), Sycrest (asenapine) and Victrelis (boceprevir) were as follows:

The explanation of terms given in the documentation was as follows:
Total
Total number of trials identified which were completed and/or with results disclosed
Unevaluable
Trials within the total which could not be evaluated (due to either trial completion date or publication date being missing or unclear) – excluded from the analysis
Evaluable
Trials with all criteria present including dates, and hence the base which could be evaluated for the assessment
Results disclosed in timeframe
Evaluable trials which fully complied with publication requirements, ie summary results disclosed (in registry or journal) within 12 months of either first regulatory approval date or trial completion date, whichever was later
Disclosure percentage
Proportion of evaluable trials which were fully disclosed
Completed before end of January 2012
Number of studies completed before end January 2012 (or already disclosed)
Results disclosed at all
Number of trials with any publication of results at any time
Disclosure percentage at 31 January 2013
Proportion of trials completed by end January 2012 which were now disclosed
* * *
The complainant listed the companies he/she would like to complain about and this included Merck Sharp & Dohme.
The complainant alleged that all of the companies listed had breached Clauses 2, 9 and 21 of the Code.
When writing to Merck Sharp & Dohme, the Authority drew attention to Clauses 1.8 and 21.3 of the Second 2012 Edition of the Code and noted that previous versions of the Code might also be relevant.
RESPONSE
Merck Sharp & Dohme stated that it interpreted the complaint as being based on the CMRO publication. The complaint did not address the registration of clinical trials but focused on alleged non-disclosure or non-timely disclosure of results. Merck Sharp & Dohme therefore confined its comments to that matter.
The objective of the CMRO publication was to produce a quantitative benchmark of disclosure rates for industry so that the ABPI and its member companies could better understand the current landscape. The ABPI used the study to highlight the positive trend of increasing levels of disclosure for industry-sponsored clinical trials, and described the study as an important milestone in demonstrating the improvements in transparency made by the industry over many years.
Merck Sharp & Dohme further noted:
- The study did not limit assessment to a single registry or to prevailing laws or requirements in specific territories and counted either posting of summary results in a clinical trial registry or publication in the scientific literature as evidence of disclosure.
- The 12 month timeframe might not meet that set out in the IFPMA Joint Position as the latter started the clock at first global marketing authorisation which was not necessarily the US or EU marketing authorisation as in the CMRO publication.
- Disclosure as marked in CMRO publication might not meet that of prevailing laws or requirements in specific territories as the publication/disclosure might not contain all the necessary information on primary and secondary endpoints etc as the CMRO publication was binary - disclosed or not.
Merck Sharp & Dohme stated that as a company fully involved with the ABPI, it supported this initiative as part of the industry’s journey to greater transparency. It submitted that the CMRO publication had applied standards that were generally accepted today, but it was important that its actions were judged by the standards applicable at the relevant time, not with hindsight.
Merck Sharp & Dohme Publication Policy
Merck & Co Inc, the parent company had a publicly stated policy on publication of clinical trial data which indicated its commitment to transparency – this policy was introduced in 2008 and had been updated. Merck’s policy for timely publication of clinical trial data was at http://www.merck.com/ research/discovery-and-development/clinicaldevelopment/Merck-Guidelines-for-Publication-ofClinical-Trials-and-Related-Works.pdf.
Jurisdiction – Timing perspective
Merck Sharp & Dohme noted that the CMRO publication included studies on its products that were completed as long ago as 2002. The studies included in the complaint relating to Merck Sharp & Dohme products included studies completed as far back as 2005. Policies on clinical trial transparency and publication had evolved, for example the 2006 Code contained no mandatory provisions relating to the publication of clinical trials. Clause 21.3 of the Second 2012 Edition of the Code referred to the 2010 IFPMA Joint Position, Clause 21.3 of the 2011 Code referred to the 2008 Joint Position and Clause 21.3 of the 2008 Code referred to the 2005 Joint Position. The CMRO publication applied standards that were generally accepted today, but it was important that Merck Sharp & Dohme’s actions be judged by the standards applicable at the relevant time and not by today’s standards and with hindsight.
Jurisdiction – International perspective
Merck Sharp & Dohme acknowledged that custom and practice in applying the Code had traditionally extended to activities of the UK operating company (wherever those activities took place) or, in the case of a subsidiary company with its headquarters outside the UK, to activities of the company’s global headquarters insofar as they were directed at UK health professionals. Application of this custom and practice would suggest that publication of studies that took place entirely outside the UK was not the responsibility of Merck Sharp & Dohme and therefore not subject to PMCPA jurisdiction. The only consideration in this regard was whether the granting of a pan-European marketing authorization amounted to directed at UK health professionals. Merck Sharp & Dohme submitted that the granting of a marketing authorisation to 26 countries was not specifically directed at any one of them and was insufficient to bring matters into scope of the Code, without specific UK involvement.
Jurisdiction – Multi-company perspective
Merck Sharp & Dohme stated finally, as noted below, it was often the case that several entities (in this case, up to five) had had responsibility for a product during the various stages of its development. The product moved from one company to another by licensing or by acquisition. Whilst each company must do due-diligence when it acquired a product, it was evidently impossible to correct a time sensitive error retrospectively. For the criterion of publication within 12 months therefore, it is seemed inappropriate to hold a company responsible for something that took place prior to its involvement in the product’s development and which could not be corrected post hoc.
Response to the complaint
The CMRO publication identified four products for which Merck Sharp & Dohme received a marketing authorisation in the time period studied, namely Elonva, Victrelis, Brinavess and Sycrest. Each product was given two scores, one relating to the ability to find publication within 12 months of study completion, the other relating to the ability to find publication at the arbitrary cut-off date of 31 January 2013.
Elonva scored 100% for each metric, and had not been included in the complaint.
For each of the remaining products, the authors provided Merck Sharp & Dohme with a list of ‘missing’ studies asking for comments. Many of those comments were subsequently provided as footnotes to the information in the electronic form of the publication.
1 Brinavess
The CMRO publication indicated that seven out of eight studies were published. The footnote in the CMRO publication indicated the company’s response: The undisclosed Brinavess trial was not sponsored by Merck Sharp & Dohme. It was a Phase II study, carried out by Cardiome Pharma Corp Inc. There was no Merck Sharp & Dohme involvement nor UK involvement. The study completed in August 2006. The study pre-dated the licensing agreement between Cardiome and Merck Sharp & Dohme in April 2009. Merck Sharp & Dohme stated that the results had been made public. This was dated June 2012.
The study was included in the dataset used by Merck Sharp & Dohme in the EU marketing authorization application, but the product was never launched in the UK, never made available to UK physicians and the marketing authorization had subsequently returned to Cardiome.
Merck Sharp & Dohme submitted that it had no case to answer under the ABPI Code. The responsibility for publishing data resided with Cardiome, the sponsor of the study. It therefore rejected the allegation of a breach of Clauses 21.3 and 9.
In response to a request for further information Merck Sharp & Dohme provided more information about the licensing agreement with Cardiome Pharma.
Secondly, the Panel requested data relating to the timeliness of publication of the Brinavess study portfolio. Data from the CMRO publication indicated that eight evaluable Brinavess studies were found of which two were identified as not published. The details were as follows:
NCT00476112
Merck Sharp & Dohme stated that this study was listed as having completed in March 2008, although the clinicaltrials.gov entry indicated a completion date of September 2004. The sponsors of the study were listed as Cardiome Pharma, with Astellas Inc as collaborators.
This study was completed long before Merck Sharp & Dohme’s involvement with the product in 2009, and could not have been published by Merck Sharp & Dohme within one year of completion. Once Merck Sharp & Dohme had acquired rights to the product, publication was prompt. There was no involvement of Merck Sharp & Dohme in the UK, nor, according to the clinicaltrials.gov entry, any UK investigators.
Merck Sharp & Dohme submitted that it should not be held responsible for the actions of other companies five years prior to its involvement in a product and therefore refuted any accusation of a breach of the Code.
NCT00267930
Merck Sharp & Dohme stated that this study related to Brinavess tablets (not the injection), a product which was dropped from development. In that sense, it had been included in the CMRO publication in error.
This study was completed long before Merck Sharp & Dohme’s involvement with the product in 2009, and could not have been published by Merck Sharp & Dohme within one year of completion. There was no involvement of Merck Sharp & Dohme in the UK, nor, according to the clnicaltrials.gov entry, any UK investigators.
Merck Sharp & Dohme submitted that it should not be held responsible for the actions of other companies five years prior to its involvement in a product and therefore refuted any accusation of a breach of the Code.
2 Sycrest
The CMRO publication indicated that all 22 clinical trials of Sycrest included in the EPAR had been published. However, only 14 out of the 22 had been published within 12 months of study completion.
Sycrest (asenapine) was a product of collaborative research between Organon Laboratories NV and Pfizer Inc. Organon Biosciences BV (the parent company of Organon Laboratories NV) was acquired by the US company Schering Plough Corporation in 2007. Schering Plough Corporation was subsequently acquired by means of a reverse takeover by Merck and Co. Inc. in 2009. Organon Laboratories Limited, the UK trading subsidiary of Organon Biosciences BV, remained an independent trading company until its assets were finally acquired by Merck Sharp & Dohme in August 2013.
Sycrest was studied for both bipolar depressive illness (manic depressive illness) and for schizophrenia. The european marketing authorization was only for bipolar illness (not for schizophrenia). The product had subsequently been licensed to Lundbeck.
All 22 studies had previously been disclosed publicly. Many of these were on the clinicaltrialresults.org web page which was hosted by PhARMA but discontinued when clinicaltrials.org was established by the FDA/NIH. The study reports were all available on the merck.com website. Merck Sharp & Dohme gave details of each of the 8 studies disclosed later than 12 months from study completion.
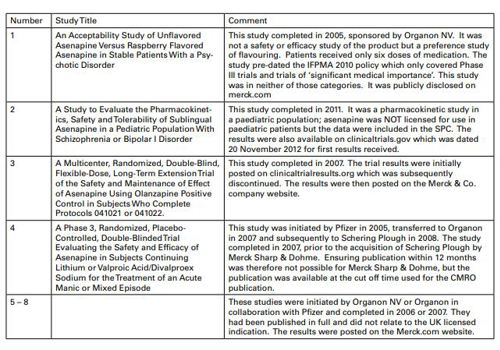
In summary, Merck Sharp & Dohme submitted that Sycrest had had a complex gestation, with five companies involved in its development and launch. All studies used to support the marketing authorization had been published. Some of these, generally relating to different pharmaceutical preparations, pharmacokinetics in sub populations or in the UK unlicensed indication of schizophrenia (rather than bipolar disorder) were not published within 12 months of completion. These studies were generally carried out in the 2005-2007 timeframe, prior to the Joint Position.
Following the acquisition of Schering Plough Corporation by Merck & Co Inc. all of the studies had been published prior to clinical availability of the product in the UK. For these reasons, Merck Sharp & Dohme rejected the alleged breach of Clauses 21.3 or 9.
In response to a request for further information, Merck Sharp & Dohme referred to the following:
Sycrest Study NCT01206517
Merck Sharp & Dohme stated that this study was a phase I clinical pharmacology study in paediatric patients. It did not address efficacy or safety as its primary objective. This was only conducted in the US. Merck Sharp & Dohme in the UK had no involvement.
Sycrest was not licensed for use in paediatric patients, only in adults. The data did not therefore relate directly to the licensed indication. Nonetheless, the data were included in the SPC.
The completion date in the CMRO publication and in clinicaltrials.gov was August 2011. The results were published in clinicaltrials.gov, dated 20 November 2012, ie 15 months after completion.
Merck Sharp & Dohme submitted that this publication was consistent with the letter and the spirit of the 2010 Joint Position, when considering that the subject matter was not of high medical or scientific importance and the data were published within 18 months of the completion. The criteria used by the CMRO publication authors were different. Merck Sharp & Dohme did not believe that categorising this as a ‘non-timely publication’ using current day expectations retrospectively amounted to a breach of the Code when judged by the standards of the time.
In response to a further request for additional information Merck Sharp & Dohme reiterated that asenapine had had a complex gestation, it was a product of research by Organon NV initially in collaboration with Pfizer. Organon NV was acquired by Schering Plough Corp. Inc. in November 2007, which in turn merged with Merck & Co Inc. This was announced in principle in March 2009 but implementation in practice as the end of 2009. In Europe, the product was then licensed to Lundbeck for commercialisation. As such, a variety of sponsors had been responsible for the clinical development at different times.
Of the eight asenapine studies, the Panel asked for specific information on six. The dates of completion and the dates of disclosure according to the legacy Organon databases that Merck Sharp & Dohme had access to were provided. Merck Sharp & Dohme also obtained information from Lundbeck, the company which now promoted Sycrest. It was possible that disclosure might have taken place even earlier, for example as a conference presentation by the investigators, but Merck Sharp & Dohme was unable to confirm this from the data available.
Only one of the six studies had UK sites. This study recruited patients from May 2005 to June 2007 and completed in December 2007. Results were presented at the 1st Schizophrenia International Research Society Conference, Venice, Italy, June 2125, 2008, and posted in December 2009 (immediately after the merger) to the (now defunct) PhRMA clinicaltrialresults.com website. They were then transferred to the merck.com website following the discontinuation of the PhRMA website. Full peer reviewed publication details were also given.
As previously noted, Merck Sharp & Dohme’s involvement in the product began in 2009 with the merger with Schering Plough. It was therefore not possible for Merck Sharp & Dohme to influence timesensitive activities prior to this time.
As noted above, this schizophrenia study did not relate to the UK indication of bipolar disorder and that the one-year definition used in the CMRO publication to define ‘timely publication’ was not the standard of the day in 2007.
Copies of conference abstracts relating to each study, which represented the first disclosure were provided.
Other activities of Organon NV and to what extent Merck Sharp & Dohme in the UK should be held responsible was considered in a previous case, Case AUTH/2363/10/10, Merck Sharp & Dohme noted that in this case which related to educational websites and not to clinical research, the Appeal Board commented ‘…in the light of the exceptional circumstances of this case, arising from successive mergers and acquisitions, Merck Sharp & Dohme and Organon NV, although part of the same global company group, were not affiliates as referred to in Clause 24.2’.
Merck Sharp & Dohme stated that it had disclosed the results of the assenapine clinical trial program as soon as it was practical to do so post-merger, consistent with Merck Sharp Dohme’s policies and commitment to clinical trial transparency. Merck Sharp & Dohme denied any breach of the Code.
3 Victrelis
The CMRO publication indicated that one of the seven studies was not published at the time of the analysis. The Merck Sharp & Dohme response was given in the footnote.
‘The trial report was submitted to the FDA within 12 month timeframe and was in the FDA review cycle. The trial results have now been made available on Clinicaltrials.gov by the FDA.’
The study was sponsored by Schering Plough and no UK involvement was known. The study completed in December 2011 and the results were published on 5 February 2013.
Merck Sharp & Dohme stated that this study showed a completion date of December 2011. Results were sent by Merck Sharp & Dohme to the US NIH [National Institutes of Health] for posting on 6 December 2012. The record was updated on 5 February 2013. In other words, Merck Sharp & Dohme had submitted the data for posting within 12 months but they were not posted by NIH until 5 days after the CMRO publication cut-off, and the trial was therefore classified as not disclosed.
In summary, this one study was submitted on time for disclosure within 12 months but because of delays in the validation process performed by NIH before posting, the publication was delayed by a few weeks. Merck Sharp & Dohme acted in good faith in submitting the data for disclosure and did not believe that this short administrative delay was sufficient to amount to a breach of Clauses 21.3 or 9.
Summary
Merck Sharp & Dohme’s submitted that its position on prompt publication was publicly stated and it strove to ensure that all activities were carried out consistent with these policies. The CMRO publication showed that the pharmaceutical industry has set itself targets, and was making great progress in achieving those targets.
Taking all four products in the CMRO publication 52 out of 54 studies had been publicly disclosed at the cut-off point. One had already been submitted and was disclosed a few weeks later. The second was a non- Merck Sharp & Dohme study and the responsibility lay elsewhere. These were the actions of a company committed to improved clinical trial transparency. Having considered all of the facts, the complex and changing nature of the data and pharmaceutical companies in control of the data, Merck Sharp & Dohme rejected the allegation of breaches of Clauses 21.3 and 9. It therefore followed that it rejected the accusation of a Clause 2 breach.
The data requested by PMCPA were extensive and Merck Sharp & Dohme believed it had provided sufficient supporting information to address the complaint. It had not provided all the data requested, such as a list of all countries worldwide in which each of the products was licenced. If PMCPA considered these essential, in reaching a decision Merck Sharp & Dohme suggested that it should be given opportunity to submit further information.
In response to a request for further information Merck Sharp & Dohme stated that the first regulatory authorisation for Sycrest was 13 August 2009 (US), Victrelis, 13 May 2011 (US) and Brinavess, 1 September 2010 (EU). The dates of commercial availability were shortly after the authorisation date in these markets.
GENERAL COMMENTS FROM THE PANEL
The Panel noted the ABPI involvement in the study. However, a complaint had been received and it needed to be considered in the usual way in line with the PMCPA Constitution and Procedure. The Panel noted that all the cases would be considered under the Constitution and Procedure in the Second 2012 Edition as this was in operation when the complaint was received. The addendum (1 July 2013 which came into effect on 1 November 2013) to this Code only related to Clause 16 and was not relevant to the consideration of these cases.
The Panel noted that the study concluded that the results of over three quarters of all company sponsored clinical trials were disclosed within a year of completion or regulatory approval and almost 90% were disclosed by 31 January 2013 which suggested transparency was now better than had sometimes been reported previously.
The Panel considered that the first issue to be determined was whether the matter was covered by the ABPI Code. If the research was conducted on behalf of a UK pharmaceutical company (whether directly or via a third party) then it would be covered by the ABPI Code. If a study was run by a non UK company but had UK involvement such as centres, investigators, patients etc it was likely that the Code would apply. The Panel appreciated the global nature of much pharmaceutical company sponsored clinical research and a company located in the UK might not be involved in research that came within the ABPI Code. It was a well established principle that UK pharmaceutical companies were responsible for the activities of overseas affiliates if such activities related to UK health professionals or were carried out in the UK.
Clause 21.3 of the Second 2012 Edition of the Code stated that companies must disclose details of clinical trials in accordance with the Joint Position on the Disclosure of Clinical Trial Information via Clinical Trial Registries and Databases and the Joint Position on the Publication of Clinical Trial Results in the Scientific Literature.
The relevant supplementary information stated that this clause required the provision of details about ongoing clinical trials (which must be registered within 21 days of initiation of patients enrolment) and completed trials for medicines licensed for use in at least one country. Further information was to be found in the Joint Position on the Disclosure of Clinical Trial Information via Clinical Trial Registries and Databases 2009 and the Joint Position on the Publication of Clinical Trial Results in the Scientific Literature 2010, both at http://clinicaltrials.ifpma.org.
The Panel noted that the first Joint Position on the Disclosure of Clinical Trial Information via Clinical Trial Registries and Databases was agreed in 2005 by the International Federation of Pharmaceutical Manufacturers and Associations (IFPMA), the European Federation of Pharmaceutical Industries and Associations (EFPIA), the Japanese Pharmaceutical Manufacturers Association (JPMA) and the Pharmaceutical Research and Manufacturers of America (PhRMA). The announcement was dated 6 January 2005.
The Panel noted that Article 9, Clinical Research and Transparency, of the most recent update of the IFPMA Code of Practice (which came into operation on 1 September 2012) included a statement that companies disclose clinical trial information as set out in the Joint Position on the Disclosure of Clinical Trial Information via Clinical Trial Registries and Databases (2009) and the Joint Position on the Publication of Clinical Trial Results in the Scientific Literature (2010). As companies had, in effect, agreed the joint positions their inclusion in the IFPMA Code should not have made a difference in practice to IFPMA member companies but meant that IFPMA member associations had to amend their codes to reflect Article 9. The Second 2012 Edition of the ABPI Code fully reflected the requirements of the IFPMA Code. The changes introduced in the ABPI Code were to update the date of the Joint Position on the Disclosure of Clinical Trial Information and to include the new requirement to disclose in accordance with the Joint Position on the Publication of Clinical Trial Results. Pharmaceutical companies that were members of national associations but not of IFPMA would have additional disclosure obligations once the national association amended its code to meet IFPMA requirements. The disclosures set out in the joint positions were not required by the EFPIA Codes.
The Panel noted that even if the UK Code did not apply many of the companies listed by the complainant were members of IFPMA and/or EFPIA.
The Panel considered that it was good practice for clinical trial results to be disclosed for medicines which were first approved and commercially available after 6 January 2005 (the date of the first joint position). This was not necessarily a requirement of the ABPI Codes from that date as set out below.
As far as the ABPI Code was concerned, the Panel noted that the first relevant mention of the Joint Position on the Disclosure of Clinical Trial Information via Clinical Trial Registries and Databases 2005 was in the supplementary information to Clause 7.5 of the 2006 Code:
‘Clause 7.5 Data from Clinical Trials
Companies must provide substantiation following a request for it, as set out in Clause 7.5. In addition, when data from clinical trials is used companies must ensure that where necessary that data has been registered in accordance with the Joint Position on the Disclosure of Clinical Trial Information via Clinical Trial Registries and Databases 2005.’
Clause 7.5 of the 2006 Code required that substantiation be provided at the request of health professionals or appropriate administrative staff. Substantiation of the validity of indications approved in the marketing authorization was not required. The Panel considered this was not relevant to the complaint being considered which was about disclosure of clinical trial results. The Joint Position 2005 was mentioned in the supplementary information to Clause 21.5 but this did not relate to any Code requirement to disclose clinical trial results.
In the 2008 ABPI Code (which superceded the 2006 Code and came into operation on 1 July 2008 with a transition period until 31 October 2008 for newly introduced requirements), Clause 21 referred to scientific services and Clause 21.3 stated:
‘Companies must disclose details of clinical trials.’
The relevant supplementary information stated:
‘Clause 21.3 Details of Clinical Trials
This clause requires the provision of details about ongoing clinical trials (which must be registered within 21 days of initiation of patients enrolment) and completed trials for medicines licensed for use in at least one country. Further information can be found in the Joint Position on the Disclosure of Clinical Trial Information via Clinical Trial Registries and Databases 2005 (http:// clinicaltrials.ifpma.org).
Details about clinical trials must be limited to factual and non-promotional information. Such information must not constitute promotion to health professionals, appropriate administrative staff or the public.’
In the 2011 Code (which superceded the 2008 Code and came into operation on 1 January 2011 with a transition period until 30 April 2011 for newly introduced requirements), the supplementary information to Clause 21.3 was updated to refer to the 2008 IFPMA Joint Position.
In the Second 2012 Edition (which came into operation on 1 July 2012 with a transition period until 31 October 2012 for newly introduced requirements), changes were made to update the references to the joint position and to include the Joint Position on the Publication of Clinical Trial Results in the Scientific Literature. Clause 21.3 now stated:
‘Companies must disclose details of clinical trials in accordance with the Joint Position on the Disclosure of Clinical Trial Information via Clinical
Trial Registries and Databases and the Joint Position on the Publication of Clinical Trial Results in the Scientific Literature.’
The relevant supplementary information stated:
‘Clause 21.3 Details of Clinical Trials
This clause requires the provision of details about ongoing clinical trials (which must be registered within 21 days of initiation of patients enrolment) and completed trials for medicines licensed for use in at least one country. Further information can be found in the Joint Position on the Disclosure of Clinical Trial Information via Clinical
Trial Registries and Databases 2009 and the Joint Position on the Publication of Clinical Trial Results in the Scientific Literature 2010, both at http:// clinicaltrials.ifpma.org.
Details about clinical trials must be limited to factual and non-promotional information. Such information must not constitute promotion to health professionals, appropriate administrative staff or the public.’
The Panel noted that in the 2014 ABPI Code the disclosure requirements which had previously been stated in Clause 21 had been moved to Clause 13.
In addition, the supplementary information stated that companies must include on their website information as to where details of their clinical trials could be found. The 2014 Code would come into effect on 1 May 2014 for newly introduced requirements following a transition period from 1 January 2014 until 30 April 2014.
The Panel examined the Joint Position on the Disclosure of Clinical Trial Information which was updated on 10 November 2009 and superseded the Joint Position 2008. With regard to clinical trial registries the document stated that all trials involving human subjects for Phase I and beyond at a minimum should be listed. The details should be posted no later than 21 days after the initiation of enrolment. The details should be posted on a free publicly accessible internet-based registry. Examples were given. Each trial should be given a unique identifier to assist in tracking. The Joint Position 2009 provided a list of information that should be provided and referred to the minimum Trial Registration Data Set published by the World Health Organisation (WHO). The Joint Position 2009 referred to possible competitive sensitivity in relation to certain data elements and that, in exceptional circumstances, this could delay disclosure at the latest until after the medicinal product was first approved in any country for the indication being studied. Examples were given.
The Panel noted that the complaint related to the disclosure of clinical trial results.
With regard to the disclosure of clinical trial results the Joint Position 2009 stated that the results for a medicine that had been approved for marketing and was commercially available in at least one country should be publicly disclosed. The results should be posted no later than one year after the medicine was first approved and commercially available. The results for trials completed after approval should be posted one year after trial completion – an adjustment to this schedule was possible to comply with national laws or regulations or to avoid compromising publication in a peer-reviewed medical journal.
The Joint Position 2009 included a section on implementation dates and the need for companies to establish a verification process.
The Joint Position 2005 stated that the results should be disclosed of all clinical trials other than exploratory trials conducted on a medicine that was approved for marketing and was commercially available in at least one country. The results generally should be posted within one year after the medicine was first approved and commercially available unless such posting would compromise publication in a peer-reviewed medical journal or contravene national laws or regulations. The Joint Position 2008 was dated 18 November 2008 and stated that it superseded the Joint Position 2005 (6 January and 5 September). The Joint Position 2008 stated that results should be posted no later than one year after the product was first approved and commercially available in any country. For trials completed after initial approval these results should be posted no later than one year after trial completion. These schedules would be subject to adjustment to comply with national laws or regulations or to avoid compromising publication in a peer reviewed medical journal.
The Joint Position on the Publication of Clinical Trial Results in the Scientific Literature was announced on 10 June 2010. It stated that all industry sponsored clinical trials should be considered for publication and at a minimum results from all Phase III clinical trials and any clinical trials results of significant medical importance should be submitted for publication. The results of completed trials should be submitted for publication wherever possible within 12 months and no later than 18 months of the completion of clinical trials for already marketed medicines and in the case of investigational medicines the regulatory approval of the new medicine or the decision to discontinue development.
Having examined the various codes and joint positions, the Panel noted that the Joint Position 2005 excluded any clinical trials completed before 6 January 2005. The position changed on 18 November 2008 as the Joint Position 2008 did not have any exclusion relating solely to the date the trial completed. The Joint Position 2009 was similar to the Joint Position 2008 in this regard.
The Panel noted that deciding which Code applied, and thus which joint position, was complicated. It noted that the 2011 Code which, taking account the transition period, came into operation on 1 May 2011 was the first edition of the Code to refer to the Joint Position 2008.
The Panel concluded that from 1 November 2008, (allowing for the transition period) until 30 April 2011 under the 2008 Code companies were required to follow the Joint Position 2005. From 1 May 2011 until 31 October 2012 under the 2012 Code companies were required to follow the Joint Position 2008. Since 1 November 2012 companies were required to follow the Joint Position 2009. The Panel considered that since the 2008 Code companies were, in effect, required to comply with the Joint Position cited in the relevant supplementary information. The relevant supplementary information gave details of what was meant by Clause 21.3 (Clause 13.1 in the 2014 Code). The
Panel accepted that the position was clearer in the Second 2012 Edition of the Code. The Panel noted that the 2011 Code should have been updated to refer to the Joint Position 2009.
For medicines first licensed and commercially available in any country from 1 November 2008 until 30 April 2011 the results of clinical trials completed before 6 January 2005 would not have to be posted.
From 1 May 2011 there was no exclusion of trials based solely on completion date and so for a product first licensed and commercially available anywhere in the world after 1 May 2011 the applicable joint positions required relevant clinical trial results to be posted within a year of the product being first approved and commercially available or within a year of trial completion for trials completed after the medicine was first available.
Decision Tree - Developed by the Panel when considering the complaint about the disclosure of clinical trial results see PDF of case report for expanded version:
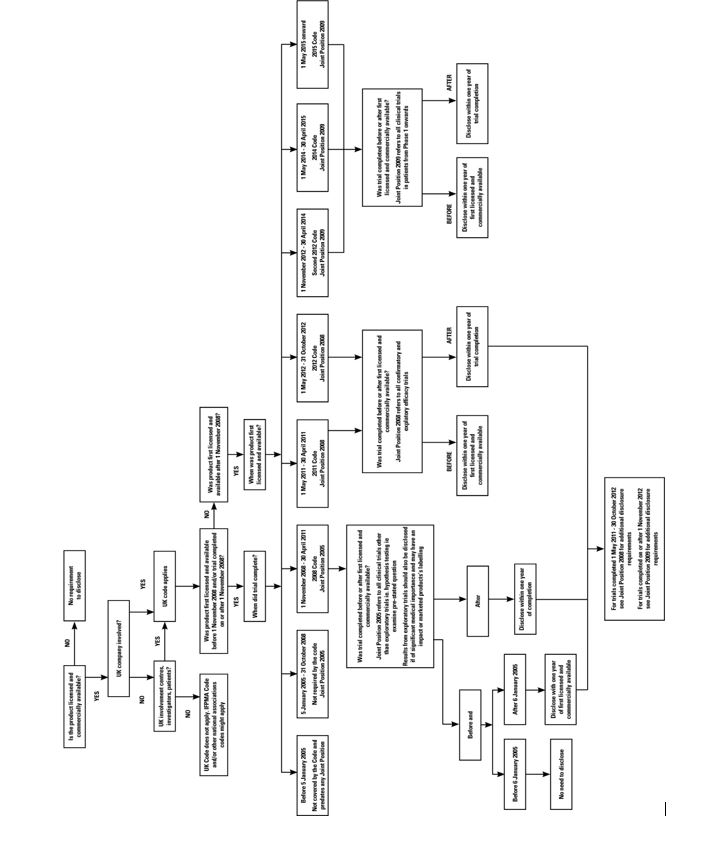
Noting that the complaint concerned licensed products the Panel considered that the trigger for disclosure was the date the product was first approved and commercially available anywhere in the world. This would determine which version of the Code (and joint position) applied for trials completed prior to first approval. The next consideration was whether the trial completed before or after this date. For trials completing after the date of first approval, the completion date of the trial would determine which Code applied. The Panel considered that the joint positions encouraged disclosure as soon as possible and by no later than 1 year after first availability or trial completion as explained above. The Panel thus considered that its approach was a fair one. In this regard, it noted that the complaint was about whether or not trial results had been disclosed, all the joint positions referred to disclosure within a one year timeframe and companies needed time to prepare for disclosure of results. The Panel considered that the position concerning unlicensed indications or presentations of otherwise licensed medicines etc would have to be considered on a case by case basis bearing in mind the requirements of the relevant joint position and the legitimate need for companies to protect intellectual property rights. The Panel followed the decision tree set out below which it considered set out all the relevant possibilities.
During its development of the decision tree, the Panel sought advice from Paul Woods, BPharm MA (Medical Ethics and Law) of Paul Woods Compliance Ltd who provided an opinion. Mr Woods was not provided with details of the complaint or any of the responses. The advice sought was only in relation to the codes and joint positions.
The Panel considered the complaint could be read in two ways: firstly that the companies listed had not disclosed the data referred to in the CMRO publication relating to the products named or secondly, more broadly, that the companies had not disclosed the clinical trial data for the product named ie there could be studies in addition to those looked at in the CMRO publication. The Panel decided that it would consider these cases in relation to the studies covered by the CMRO publication and not on the broader interpretation. Companies would be well advised to ensure that all the clinical trial results were disclosed as required by the Codes and joint positions. The Panel considered that there was no complaint about whether the results disclosed met the requirements of the joint positions so this was not considered. In the Panel’s view the complaint was only about whether or not study results had been disclosed and the timeframe for such disclosure.
The CMRO publication stated that as far as the IFPMA Joint Position was concerned implementation had been somewhat variable in terms of completeness and timing. The Panel noted that a number of studies were referred to in the CMRO publication as ‘unevaluable’ and these were not specifically mentioned by the complainant. The CMRO publication focussed on the disclosure of evaluable trial results and the Panel only considered those evaluable trials.
The Panel noted that its consideration of these cases relied upon the information provided by the respondent companies. The CMRO publication did not identify the studies evaluated; it only provided quantitative data. The Panel noted that the study ran from 27 December 2012 to 31 January 2013 and was published in November 2013. The Panel considered that companies that might not have been in line with various disclosure requirements had had a significant period of time after the study completed and prior to the current complaint being received to have disclosed any missing information. It appeared that the authors of the CMRO publication had contacted various companies for additional information.
The Panel noted that the case preparation manager raised Clause 1.8 of the Second 2012 Edition with the companies. The supplementary information to
Clause 1.8, Applicability of Codes, inter alia, referred to the situation when activities involved more than one country or where a pharmaceutical company based in one country was involved in activities in another country. The complainant had not cited Clause 1.8. The Panel noted that any company in breach of any applicable codes, laws or regulations would defacto also be in breach of Clause 1.8 of the Code; the converse was true. The Panel thus decided that as far as this complaint was concerned, any consideration of a breach or otherwise of Clause 1.8 was covered by other rulings and it decided, therefore, not to make any ruling regarding this clause (or its equivalent in earlier versions of the Code).
PANEL RULING IN CASE AUTH/2672/11/13
The Panel noted Merck Sharp & Dohme’s submission regarding the industry’s move to greater transparency. It considered that this was reflected in the establishment and development of the Joint Positions and the inclusion and development of requirements in the ABPI Code and other codes. In reaching any decision the Panel always took into account the dates of the codes and other relevant documents.
The Panel noted that Merck Sharp & Dohme submission that some studies published in 20052007 were prior to the first Joint Position (published on 6 January 2005) and was clear that the results of relevant clinical trials which completed after 6 January 2005 were to be disclosed. The Panel noted that as set out above the date a product was first approved and commercially available would determine which Joint Position applied and thus whether studies completed between 2005 and 2007 needed to be published.
The Panel noted Merck Sharp & Dohme’s comments about marketing authorisations. It did not consider that whether a product had a UK marketing authorization or not was relevant to the need to publish. As set out above the relevant factors were whether the trial was run by the UK company or had UK involvement. The Panel considered each product separately.
1 Brinavess
The Panel noted that two of the evaluable studies had not been disclosed in the timeframe. The disclosure percentage was 75%. One study completed before the end of January 2012 had not been disclosed. The disclosure percentage at 31 January 2013 of trials completed by the end of January 2012 was 88%. A footnote explained that the undisclosed trial was not sponsored by Merck Sharp & Dohme; it was sponsored by Cardiome.
The Panel noted that both studies were sponsored by Cardiome and not Merck Sharp & Dohme. It appeared from the information provided by Merck Sharp & Dohme that the results for one study were disclosed in June 2012 and that the other was not on the licensed presentation. The Panel considered that as far as Merck Sharp & Dohme was concerned the matter did not come within the scope of the Code and therefore ruled no breach.
2 Sycrest
The Panel noted that eight of the evaluable studies had not been disclosed in the timeframe. The disclosure percentage was 64%. The disclosure percentage at 31 January 2013 of trials completed before the end of January 2012 was 100%.
The Panel considered that Merck Sharp & Dohme was responsible under the Code for publication of Organon and Schering Plough studies.
The Panel noted Merck Sharp & Dohme’s submission that Sycrest was first approved on 13 August 2009 and became commercially available shortly thereafter. For studies completed before that date the 2008 Code applied and hence the Joint Position 2005 was relevant.
The Panel noted that study one completed in 2005. It was not clear when the results were posted or whether there was UK involvement. The study was a preference study of flavouring, The Panel considered that this study could be considered an exploratory trial and thus the results did not need to be disclosed under the Joint Position 2005 unless they were deemed to have significant medical importance and might have an impact on product labelling. The Panel was unsure whether the results were of significant medical importance. The complainant had not provided any details in this regard. The Panel considered that publication of such data was preferable however on the information before it there appeared to be no need to disclose the trial results under the 2008 Code. The Panel ruled no breach of Clause 21.3 of the 2008 Code and consequently no breach of Clauses 9.1 and 2.
Another study completed in 2011 but was a pharmacokinetic study for an unlicensed indication. The Panel noted Merck Sharp & Dohme’s submission that this study was on an unlicensed population and the data were included in the summary of product characteristics. In addition, it appeared the results were posted on clinical trials.gov in November 2012. Merck Sharp & Dohme submitted there was no UK involvement. The Panel considered that as there was no UK involvement the matter did not come within the scope of the Code and therefore ruled no breach.
The Panel noted Merck Sharp & Dohme’s submission that five of the remaining six studies had no UK involvement identified and that the trial results had been disclosed. The Panel considered that as there had been no UK involvement the matter did not come within the scope of the Code and therefore ruled no breach.
The Panel noted Merck Sharp & Dohme’s submission that the final study completed in December 2007. Results were presented at a meeting in June 2008 and posted in December 2009 immediately after the merger. The trial had UK sites. The Panel noted that the trial was on an indication unlicensed in the UK but schizophrenia was licensed in the US so the trial was covered by Joint Position 2005. The trial needed to be disclosed within one year of first approval and commercial availability of Sycrest ie before August 2010. On the information submitted by Merck Sharp & Dohme it appeared that this had been done as the study was posted in December 2009. The Panel therefore ruled no breach of Clause 21.3 and consequently Clauses 9.1 and 2 of the 2008 Code.
3 Victrelis
The Panel noted that one of the evaluable studies had not been disclosed in the timeframe. The disclosure percentage was 86%. The disclosure percentage at 31 January of trials completed before the end of January 2012 was 100%. A footnote stated that the report was submitted to the FDA within the 12 month timeframe and was in its review cycle and that the trial results had been made available on clinical trials.gov by the FDA.
The Panel noted that Victrelis was first approved and commercially available in May 2011. It also noted Merck Sharp & Dohme’s submission that it did not know of any UK involvement in the study. The study completed in December 2011 and the results disclosed in February 2013. The Panel considered that as there was no UK involvement the matter did not come within the scope of the UK Code and therefore ruled no breach.
Complaint received 21 November 2013
Case completed 20 March 2014
see cases: 3005,2908,2906,2903,2898,2763,2676,2674,2673,2672,2671,2670,2669,2667,2666,2665,2664,
2663,2662,2661,2659,2657,2654